Hey, there! Log in / Register

Preliminary data show coronavirus hitting blacks in Boston more than other groups
By adamg on Fri, 04/10/2020 - 12:01am
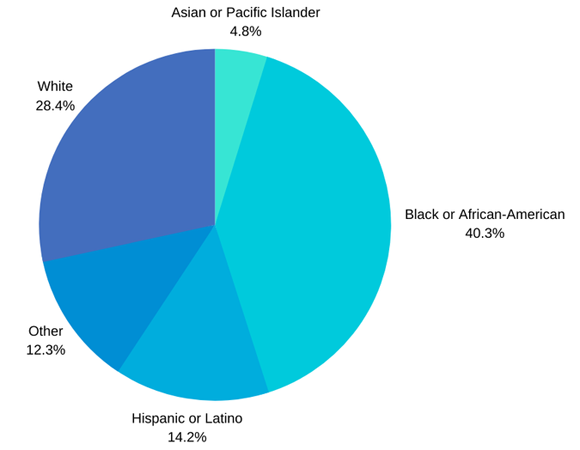
Boston today released preliminary Covid-19 data that show some 40% of the patients are black, even though blacks make up only 23% of the city population.
And while citywide figures show the percentage of Latino patients is lower than the Latino proportion of the overall city population, Massachusetts General Hospital reports that 40% of its Covid-19 patients speak Spanish as their native language - significantly higher than the hospital's usual patient census. Mass .General is the closest hospital to East Boston, which has a large Spanish-speaking population - and which the Boston Public Health Commission said last week had a higher rate of cases than the citywide average.
The caveat with the data is that roughly 38% of the city's 2,812 confirmed Covid-19 cases are currently marked as unknown for racial or ethnic background. But the numbers, when combined with higher-than-average numbers in East Boston, Dorchester, Mattapan and Hyde Park, are significant enough that Mayor Walsh today announced a COVID-19 Health Inequities Task Force to figure out what to do about them.
In a statement, Walsh said:
We know that there are significant inequities that put our communities of color and immigrant population at higher risk for contracting coronavirus, developing severe illness, and impeding them from accessing care.
The city also cited data from Boston Medical Center:
Of patients where race is reported, 80% of COVID-19 positive patients are either black or Hispanic/Latino, compared to 58% historically. Additionally, 61% of COVID-19 positive patients are from Dorchester, Roxbury, Hyde Park and Mattapan, compared to 44% historically. Many of BMC's COVID-19 positive patients have presented with higher rates of underlying conditions compared to historical data, including 34% with diabetes, 49% with hypertension and 52% with a Body Mass Index above 30.
The members of the new task force are:
Dr. Thea James, Boston Medical Center; Vanessa Calderón-Rosado, IBA; Manny Lopes, East Boston Health Center; Guale Valdez, Mattapan Community Health Center; Carol Rose, ACLU; Alexandra Oliver-Dávila, Sociedad Latina; Frederica Williams, Whittier Street Health Center; Michael Curry, Mass League of Community Health Centers; Dr. Joseph Betancourt, MGH; Karen Chen, CPA; Tanisha Sullivan, NAACP; Michele Courton Brown, Quality Interactions; Rev. Ray Hammond, Bethel AME Church; Rev. Gloria White Hammond, Bethel AME Church; Paul Watanabe, UMass Boston; Dr. Lorna Rivera, UMass Boston; Suzanne Lee, former principal, Josiah Quincy School; Eva Millona, MIRA Coalition; Marie St. Fleur, St. Fleur Communications, former State Representative; Rev. Sam Acevedo, COPHANI; Petrina Cherry, Boston Medical Center; Linda Dorcena Forry, Suffolk Construction; Dr. Jean Alves, Bowdoin Street Health Center; and Dr. Myechia Minter-Jordan, DentaQuest Partnership for Oral Health Advancement.
Boston at a glance: 2020 - BPDA report that has racial/ethnic breakdown of Boston population.
Neighborhoods:
Free tagging:
Ad:
Support Universal Hub
Help keep Universal Hub going. If you like what we're up to and want to help out, please consider a (completely non-deductible) contribution.
Comments
Discussion of these issue in NYC in NYT
Article talking about the problems in poor areas, minority and/or immigrant, in NYC that is largely applicable here as well. Not behind a paywall.
https://www.nytimes.com/2020/04/09/nyregion/coronavirus-queens-corona-ja...
since the posting mentions
since the posting mentions mattapan, dorchester, hyde park are haitians considered latine or black or both (i assume just black but not latine) ?
so in this case i think latino just means hispanic and not franco-fone.
normally it doesnt matter but for this statistic the overlap mite be significant.
Just black
Haitians- like African Americans, Nigerians, and Jamaicans are just black, not latino.
This is a strange pie
The Census Bureau defines "Hispanic or Latino" as "a person of Cuban, Mexican, Puerto Rican, South or Central American or other Spanish culture or origin regardless of race."
A person can be Latino and Black. Latina and white. Hispanic and neither Black nor white. Hispanic and AAPI.
Bad chart! No dessert!
yeah it becomes tuff to
yeah it becomes tuff to quantify becuz hispanic is technically not a race.
I wonder
How many of the victims were regular riders of the petri dish of germs otherwise known as the MBTA.
Nursing home workers.
Based on my own empirical observations, 90% plus of nursing care and assisting living facilities are staffed by black workers. And these black workers are very susceptible to getting something like Covid-19 for obvious reasons. We have also obviously seen huge outbreaks in Covid in pretty much every nursing home in Boston, and I'm not sure that is because of testing there, or because it is more under a microscope, but I was just thinking that nursing homes may be a huge factor in this.
There are so many factors that need to be looked at here. Do whites have greater access to tests? What is breakdown of % by race for tested:positive/negative? Are certain racial groups able to get tests through their primary care physician based on their health care plans? Are certain groups waiting until they get too sick because they don't have good health care plans?
Do all hospitals have the same protocol in how they deal with testing and Covid Patients? That right there could be a factor. You have the BI, Brigham, St. E's and Faulkner on "one side" of Boston, with BMC, and Mass General on the other side. Are these hospitals balanced out? Do they treated patients with Covid symptoms the same? Are Randolph residents at BMC included in these stats? Would be interesting to see the racial/general breakdown by hospital as well. Boston EMS will often transport patients by emergency room availability, and I'm sure they have a new protocol for this as well.
Nursing homes and now it’s
Nursing homes and now it’s Amazon as one of the Main contributors from its staff to drivers to the infected items that they deliver to homes.
Vitamin D?
https://thorax.bmj.com/content/67/11/1018.full
https://www.ncbi.nlm.nih.gov/pubmed/32252338
https://www.ncbi.nlm.nih.gov/pubmed/16549493
Maybe, but likely not
Social determinants of health are among the strongest predictors of whether or not someone experiences ill health.
Things like poverty, racism, and language barriers.
Dr. Monica Bharel talks often of how she would give the standard health advice to her patients at an urban clinic, only to get completely schooled on the reality of the barriers to following that advice (two jobs, no car, rough neighborhood, limited access to healthy food).
https://www.mass.gov/social-determinants-of-health...
.
Hoofbeats = horses, not zebras
Unfortunate yet natural progression
This largely makes sense. The pandemic started among wealthy people - e.g., people traveling internationally and, locally, the Biogen conference to which people traveled to and from. After all, people who travel internationally have a certain amount of wealth to do so. Scientists who work at Biogen are also wealthy. Early on cases in Boston were in more affluent parts of the city.
Once social distancing starts, the more affluent have more space to themselves to retreat to. Any number of minority workers who work essential jobs - first responders, nursing homes, MBTA, supermarket workers, etc - who also live in less affluent areas are going to suffer more. The minority neighborhoods hardest hit have denser housing and multigenerational family housing. That's a recipe for the virus to spread.
The outlier seems to be Hyde Park. While HP has some sections that have denser housing, HP as a whole also has more space.
That being said, it's also hard to rely on this data when it's only representative of 38% of the confirmed cases. That's compounded by FDA and CDC failures early on that resulted in unreliable data in almost every context. We'll never know how many cases actually exist.
more space to themselves to retreat to? not entirely true...
if you check the actual data - you will see that middlesex county (with lots of affluent areas and plenty of "space to themselves to retreat to" as you put it.) account for just as many cases as in Suffolk County. But don't let that destroy your race based narrative.
Data's a funny thing ...
Middlesex County has roughly twice as many residents as Suffolk County, so why are you surprised at how many cases it has? If anything, based on such a simplistic argument as yours, you'd expect it to have closer to twice as many cases as Suffolk County (it's also not quite all leafy white-bread burbs, but maybe you've never been to Framingham or Lowell - or even Cambridge and Somerville).
Realistically, what can the
Realistically, what can the "COVID-19 Health Inequities Task Force" do, besides point out that inequities exist?
We may be in the sprint
We may be in the sprint portion of the race now but this is a marathon that goes 18 months or longer... so they have to plan long and short term. Short term they need to look at which communities are getting benefits and which are not. These $1,200 checks are great and all but if you and your wife/husband (or if you are single mom etc) were to lose your jobs and now prices for basic items are expensive and the local store has no food so you have to order it at a markup. It all adds up. So in the short term we need to make sure that is addressed.
In the long term we have to figure out how to deal with this issue. Better access to healthcare, easier cheaper access for these communities. Also once you pinpoint where the problem is you can work with leaders from those communities on how to get the message across while listening to what the underlying problems are.
We can scream until we are blue in the face to STAY HOME but then we sit back and order booze from Drizzly and a pizza from the local pizza shop. Who do you think is stocking, making and doing these things? A ghost?
Well...
...they can make recommendations for where testing and treatment should be focused. Don't you think that's worth something?
Realistically?
First, ignore people like you who don't really give a shit anyway.
Second, try to figure out why the rate is so high and do something about it. Are people not getting the message about social distancing? Are they getting the message but feel they have no choice but to risk their lives to keep working at their "essential" jobs to feed their families? Are rates rising because people are crowded into multi-family buildings? And then, once you figure out the issue or issues, you come up with a strategy to combat them.
Classic example of "Doing Something" just to do
Unless the whole is just a -- "I'll name some people to some euphonious sounding committee" -- which may or may not eventually issue a report which absolutely no-one will read -- Otherwise this is an absolute waste of time and other resources
We know that anyone can get COVID-19 by being exposed to a source of the SARS-COV-2 virus -- irrespective of any known factors such as age, sex, height, weight, skin-type, race, ethnicity, income, location, occupation, environmental factors
We also know because of the protocol until recently -- that almost all who are tested either so-sick that they end up in a hospital or they are an EMT, etc.
We also know that many of the poor and especially minority poor have less beneficial life-styles [such as poor diets, obesity, smoking] leading to more of the co-morbitity factors that make COVID-19 much more serious [e.g. Asthma, diabetes, cardiovascular disease, renal disease]
Finally, there are the contact factors providing enhanced opportunity to be close to infected individuals -- many minority people work in jobs which are likely to expose them to lots of potentially infected people -- such as working in a nursing home, working as an EMT, supermarket cashier, bus driver, etc. There is also a greater number of minority young adults who participate in contact-sport type of recreation [e.g. highly competitive basketball]
I doubt that the vaunted panel will find anything other than the above -- but it might give some people some "feel-good" points
i love that
you wrote nearly 10 paragraphs that amount to “lol black people are poor and they love basketball” and thought it profound enough to post
Just shut up
DPH has been intensely focused on disparities in health since Bharel took the helm.
You are spewing ignorance, and too ignorant to even understand how ignorant it sounds
If it is no surprise that the usual disparities are causing the usual misery, that does not mean that it isn't important to document it ... IT MEANS THAT IT IS TIME TO FUCKING DO SOMETHING ABOUT THE DISPARITIES AND KEEP IT UP.
https://www.mass.gov/files/2017-08/vision-and-mission.pdf
False rumors that "blacks can't get it" fueled complacency
For starters, many blacks were misled into complacency by a widely circulated false rumor stating that "blacks can't get it." This was bolstered by low (reported) rates in Africa despite large numbers there traveling/trading with China. Epidemiologists feared a major outbreak in Africa would be devastating due to the lack of basic care/ventilators in remote areas. The early maps showed that wasn't happening. So without question, some blacks didn't take early precautions and even joked about their perceived immunity. As for the BMC numbers, based on location, insurance and demographics, it's understandable they would be higher than the "elite" hospitals.
I'm also reminded of one of Ted Koppel's best moments on his pioneering ABC Nightline show. In 1987, when an L.A. Dodgers executive (quickly fired) raised the old, racist trope "why aren't blacks good swimmers?" Koppel shot back, "maybe because they don't have access to the country clubs and pools." 33 years later and many blacks still don't have access to the best health insurance and the suburban supermarkets carrying Purel, Clorox wipes etc. While I believe the numbers, there could be many reasons for them.
Repeating uninformed ideas and rumors caused issues?
Huh, I wonder why you're still commenting here then.
Mixing race and ethnicity
You are mixing race and ethnicity in same pie chart. I agree: no dessert for you.