
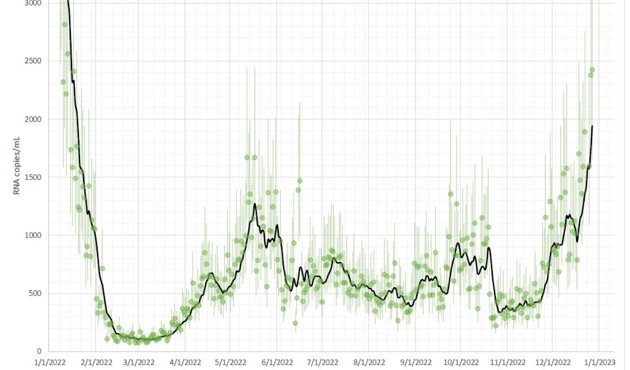
The latest numbers from the MWRA's Deer Island treatment plant are out and they're not looking good.
The numbers, which show how much of the virus is being excreted by MWRA customers in Boston and other parts of the area, have become a predictor of actual Covid-19 diagnoses seven to ten days out. But even before that, our Covid hospitalization numbers are on the rise as well, Jon Levy, chair of environmental health at the BU School of Public Health, reports:
Boston-area wastewater levels are where they were in early Jan and rising fast. MA COVID hospitalizations are at highest since winter Omicron wave, with > 100 COVID deaths last week for the first time in a long time. Little public acknowledgment. We have become comfortably numb.
BPS today announced eight school days of indoor masking, but said nobody will be penalized for refusing to put on a mask.
Like the job UHub is doing? Consider a contribution. Thanks!
Ad:
Comments
Crap
By JJ
Fri, 12/30/2022 - 11:35am
Literally.
(edit: should explain I mean "crap" as in the exclamation. not implying the data is "crap". well it is crap literally but not figuratively. what was I saying again?)
BPS masking
By emac
Fri, 12/30/2022 - 12:46pm
BPS will “ask and expect” (but not mandate or punish non-participants) students and staff to mask for the first two weeks. Which: good. As they point out in the announcement, January 2022 averaged nearly 20% absence amongst students and such short staffing that schools could barely stay open, at our own school the family liaison was teaching classes. Hopefully with a bit of prevention we can avoid that disruption again.
https://www.wcvb.com/amp/article/boston-public-schools-adopts-temporary-...
This is what every post Xmas will look like…
By tblade
Fri, 12/30/2022 - 2:20pm
…for a long time.
Who gives a shit!
By Tipsdown
Fri, 12/30/2022 - 3:02pm
Who gives a shit!
(No subject)
By SwirlyGrrl
Fri, 12/30/2022 - 9:20pm
[img]https://www.joeydevilla.com/wp-content/uploads/202...
Not just covid
By mg
Fri, 12/30/2022 - 3:27pm
Hospitals are currently overflowing with cases of flu, RSV, and Covid and there's a real shortage of pediatric beds. As anyone who's had kids or had co-workers with kids knows, schools are hotbeds of germ transmission and kids are generous at sharing with family who then share with others in their offices.
Masking is protective against viruses and bacteria in general. Wearing a mask both protects you from catching things and also protects people around you from catching anything you may currently be infectious for, whether or not you are symptomatic yet.
We used to “flatten the curve”
By Waquiot
Fri, 12/30/2022 - 4:50pm
But 2+ years of attempting (and failing) to stop Covid means the kiddos are catching up on 2 winters without exposure to the everyday germs that are a part of growing up. What is happening with flu and RSV now is inevitable. If we were taking the same precautions this winter that we took last winter, everything would be delayed until next year, with worse results.
Do I know you?
By SwirlyGrrl
Fri, 12/30/2022 - 9:21pm
Are you in public health?
Or are your "theories" your own?
Lol
By emac
Fri, 12/30/2022 - 9:50pm
man with opinions, god forbid he keep those to himself.
Opinions?
By Bob Leponge
Sat, 12/31/2022 - 12:03pm
Assertions about how the immune system works are not “opinions.” They have an objective truth value that can be deduced from data. Such statement are either consistent with the existing body of observed data ir inconsistent with the existing body of observed data.
You pontificate on the Catholic Church, no?
By Waquiot
Fri, 12/30/2022 - 11:07pm
But in my case my views come from reading and watching numerous reports on the uptick.
But I'm sure you can enlighten us with the real reason why, after 2 quiet winters, RSV and influenza are back with a vengeance. Here's an article on RSV, in case you haven't been keeping up with things. It also mentions influenza.
Any thoughts on China's second wave of Covid while we're at it?
Nah, it's immune system damage from COVID
By Mjolnir
Sun, 01/01/2023 - 11:24am
"What doesn't kill you makes you stronger" is not an accurate summary of viral epidemiology. Why would you need an updated flu shot every year if getting exposed to the flu in 2020 would protect you from the flu in 2022? They studied immunity from RSV in the 1990s and it's certainly not 2+ years of protection: "By 2 months about one-half and by 8 months two-thirds of the subjects became reinfected." Plus, while the US never really had an enforced and policed "lockdown" such as China, some countries like Sweden proudly never had any real restrictions or mandates of any kind from day 1 - and they're seeing the same massive wave of pediatric sickness, including in "samma barn i år som förra året" - the same children this year as last year. You can also see that we in the Northeast had plenty of sickness last year - Rhode Island for instance had no RSV in 2020, but they had as much or more RSV in 2021 than in 2018-2019, and still had a massive wave this year that strained the hospitals.
Meanwhile, there is substantial evidence that COVID infection damages your immune system for months and thereby makes you more susceptible to other infections.
[quote][b]Texas Public Radio: Is immunity debt or immunity theft to blame for children's respiratory virus spike?[/b]
At first, some people theorized that the tools used to protect against COVID-19, like isolation and masking, had left children vulnerable to other infections. The theory is called immunity debt, and it suggests that because children's immune systems hadn't been challenged by viruses like respiratory syncytial virus — RSV — while taking protective measures against COVID, they had become more susceptible to infection.
However, the immunity debt theory doesn’t seem to hold up to scrutiny. Dr. Tess Barton, UT Health San Antonio associate professor of pediatric infectious diseases, understands where the idea came from.
“The nugget of truth in there is that we do build immunity over time with repeated exposures to things," Barton said. "So, getting exposed to things does help us to build up our immune system.”
But this is the second real RSV season we’ve had during the pandemic, with a big surge during the summer of 2021, Barton said.
“That was sort of the great unmasking, and everybody got viral illnesses," she said. "Now we're past that. We've already been through that. We should have some immunity from that, and we're having it again.”
Barton also pointed out that many of the people getting sick this fall weren't even born when people were taking precautions against COVID infection.[/quote]
That article goes on to explain the immune damage being caused by COVID. Here's some other mainstream reporting:
[quote]Financial Times: ‘Immunity debt’ is a misguided and dangerous concept
That has fuelled speculation that pandemic mitigations, including lockdowns, created a harmful “immunity debt”, with children left vulnerable through a lack of exposure to the usual cut and thrust of viral infections. But scientists have dismissed the concept, as applied to individual immunity, as misguided.
The discussion swirling around immunity debt shows how easy it is for a plausible-sounding theory to circulate as misinformation. In this case, misinformation risks promoting the unfounded assertion that infections are clinically beneficial to children, as well as feeding the revisionist narrative that Covid measures did more harm than good.[/quote]
[quote]The Guardian: Does exposure to cold and flu viruses weaken or strengthen the immune system?
Besides the risk of long Covid, there is mounting evidence that Sars-CoV-2 may have a negative impact on the immune system for weeks or months after the infection has subsided. For instance, recent research by Akiko Iwasaki, at the Yale School of Medicine in New Haven, Connecticut, has identified an altered balance of circulating immune cells in people with long Covid.
Dunn-Walters said: “They are showing lots of changes that aren’t what I would call strengthening the immune system. Rather, Covid-19 appears to be skewing the immune system in not a very good way, meaning people may not be able to react to other infections as well.”
An article in Nature Communications this week reported on evidence that exposure to Sars-CoV-2 may reduce the diversity of bacteria in our guts, potentially creating space for antibiotic-resistant microbes to thrive. “Our results highlight how the gut microbiome and different parts of the body’s immune system are closely interconnected. An infection in one can lead to major disruptions in the other,” said the study’s author, Dr Jonas Schluter, at NYU Langone Health, in New York.[/quote]
[quote]Global News Canada: ‘Immunity debt’: Why experts say this new term promotes COVID-19 ‘misinformation’
But this notion that governments and public health officials have been “coddling” the public’s immune systems by wearing masks and staying home and that this has eroded people’s immunity to other viruses like influenza or respiratory syncytial virus (RSV) is simply not true, says Colin Furness, an infection control epidemiologist and assistant professor in the faculty of information at the University of Toronto.[/quote]
Some peer-reviewed scientific papers from major journals have documented many types of immune damage. For instance:
And much much more. The data is out there. This Twitter thread compiles some more.
Ever read about the influenza outbreak of 1918?
By Waquiot
Sun, 01/01/2023 - 10:28pm
It affected an age group typically not affected by influenza. But you know the reason why, so I won't insult you by dredging that up.
I do indeed
By Mjolnir
Mon, 01/02/2023 - 9:11am
It's because scientifically-illiterate and/or selfish people didn't wear face masks that help prevent the spread of a novel, deadly, airborne pathogen, despite medical science at the time communicating clearly it was an important aspect of public health in such a scenario.
[img]https://i.imgur.com/VXvfJB3.jpg[/img]
So you missed the part
By Waquiot
Wed, 01/04/2023 - 10:18pm
Where a segment of the population that is usually relatively unaffected by influenza was disproportionately affected by the virus.
Unclear what you're getting at
By Mjolnir
Wed, 01/04/2023 - 10:31pm
I didn't miss that part? The virus that caused the 1918 pandemic was more deadly than previous local influenza strains, so it killed more people, and more diverse groups had worse outcomes. Similarly, SARS-CoV-2 is a very nasty coronavirus, much more so than our typical "common cold" coronaviruses, so it harms more people, and harms them more. Quod erat demonstrandum.
You should study the outbreak
By Waquiot
Sat, 01/07/2023 - 10:52pm
Unlike other influenza outbreaks, the 1918 outbreak affected people aged 20-40 disproportionately. One of the reasons given for this is that the 20-40 cohort had missed exposure to similar influenza strains when they were younger. Again, more kids are catching RSV this season because they didn't the previous 2 seasons. Long term, this will even out, but this is what we are seeing this year.
If you ever get curious about pandemics, I recommend The Great Influenza by John Barry. Here's something from 2012 on the theory.
That doesn't say what you think it says
By Mjolnir
Sun, 01/08/2023 - 9:03am
The 2012 paper you posted suggests one hypothesis that says:
This means that people who had developed acquired immunity to a previous influenza strain, when then exposed to the 1918 flu strain, had an inappropriately strong T cell driven immune response, causing self-inflicted harm to the body which made these people vulnerable to other unrelated pathogens such as bacteria. Consistent with this theory, if those people had masked in 1889 and avoided exposure to that particular influenza strain, they would have had BETTER outcomes during the 1918 pandemic, even if they got infected at that point.
To be clear, post-covid immune hyperactivation followed by T cell exhaustion leading to inhibited immune responses to future pathogens is one of the things being reported in the links in my original post. And this will be exacerbated, not reduced, by additional rolling waves of COVID, flu, and RSV infection every year.
If nobody in MA had RSV for two years and getting RSV will fix the issue, why did they have it last year and then have it worse this year? What do you think about the RI data I posted? Or that Swedish children's hospitals are seeing the same kids two years in a row? To paraphrase the experts like pediatric immunologists in the recent articles I posted earlier, getting infected with a virus is never a good and helpful thing - it's a bad thing that causes harm, and those harms can interact and compound, as demonstrated by that 2012 article you yourself posted.
Mainstream reporting now catching up
By Mjolnir
Thu, 03/30/2023 - 12:00pm
And the Red Sox lost today
By Waquiot
Thu, 03/30/2023 - 5:42pm
Which also has nothing to do with influenza.
Still, with hindsight we know that the rising hockey stick, while bad, was a lapping wave compared to the tsunamis of Feb-Apr 2020 and the winters of 2020-21 and 2021-22.
Take the L, buddy.
By Mjolnir
Mon, 04/24/2023 - 10:45am
You posted:
That paper you linked says:
That says [b]THE EXACT OPPOSITE OF YOUR CLAIM[/b]. It doesn't hypothesize that young healthy people suffered from the 1918 pandemic because they "missed exposure to similar influenza strains"; it says explicitly that HAVING a previous exposure to a similar influenza strain screwed them over, by creating "immunopathologic effects of the dysregulated T-cell response" which "transiently increased susceptibility" to completely different infections.
[b]As we are also seeing now[/b], in situations like the Candida auris surge and other opportunistic infections like Streptococcus constantly hitting adults and children (due to their damaged immune systems post-COVID).
Did I really lose?
By Waquiot
Wed, 04/26/2023 - 10:41pm
As you are insisting on commenting on an article from months ago, I'd say we have the benefit of hindsight. Hindsight tells us that the winter of 2022-23 wasn't too bad at all in terms of infectious diseases. That makes all of us winners, assuming you didn't bet your mortgage that it was going to be as bad as you thought it was going to be. That would have made you a very big loser.
Did you ever read the book I recommended you?
"Wasn't too bad" vs...?
By Mjolnir
Thu, 04/27/2023 - 11:58am
We're still suffering from significantly higher excess deaths compared to before the pandemic. We've stopped testing for COVID and reclassified what counts as a COVID death between the waves, comparing apples (winter wave 2021/22) to oranges (22/23). Rather than dying acute deaths, people are getting strokes and heart attacks months or years after infection as even mild COVID can lead to arterial stiffness and increased blood pressure. And as I linked to in the post you're replying to, we've now been experiencing waves of deadly bacterial and fungal infections capitalizing on our newly-immunosuppressed population.
Did you ever read the paper you recommended to me?
Turns out, you were kind of right!
By Mjolnir
Mon, 09/11/2023 - 7:57am
Saw this and it reminded me of the paper you posted (but apparently didn't read first) with a similar hypothesis about the 1918 flu pandemic, which is that previous exposure to similar virus strains can make your response to the new virus worse:
The Covid-19 vaccines should've been made mandatory.
By mplo
Tue, 01/03/2023 - 6:25pm
A huge part of the problem is due to the fact that the Covid-19 vaccines, unlike polio vaccines and other vaccines, were not made mandatory for everybody who was able to get the Covid-19 vaccinations from the beginning. Thanks to the anti-vaxxers, and the anti-Covid-19 vaxxers, and thanks to ex-President Donald Trump, we're not even close to being out of the woods yet.
Had the Covid-19 vaccinations been made mandatory from the beginning for everybody, regardless of age who was able to get those vaccines, we'd be out of the woods and back to normal, or at least close to it, by now.
Unfortunately, I'm not sure
By Mjolnir
Wed, 01/04/2023 - 9:26am
While I don't disagree with you that mandating them may have been the best public health option available at the time and objectively better than what we did instead, I'm not sure that could have gotten us back to normal.
1) When they were first being deployed, there simply wasn't enough vaccine available for everyone at the same time. As you remember, there were months of priority tiers because supply was legitimately constrained. However, there was a lot of interest and sharp voluntary uptake of the vaccines through the Spring, until we hit around the 50% mark nationally. Mandates could have kept that uptake rate constant for the rest of 2021, except...
2) Vaccine efficacy wanes, quickly. The mRNA vaccines are extremely effective at rallying an intense immune response fast and if you were 2 weeks out from your 2nd shot in the Summer of 2021, you were basically invulnerable from COVID - but protection from infection really only ever lasted 4-8 months or so, and protection against hospitalization and death wanes some time after that. I "bandited" my first booster in late summer 2021 because they weren't broadly approved, but the neutralizing antibody data (Pfizer's own, as well as Israeli population data) was extremely clear that they stop working against infection fast. Besides acute death there are many reasons you'd want to avoid a survivable, mild COVID infection - such as the development of Long COVID, ME/CFS, increased risks for sudden heart attacks and strokes which can happen for a year or more after infection, the immune system damage outlined above, increased risk of developing diabetes, etc. So you can't just immunize everyone once, you have to immunize everyone AT once, or within a pretty short timeframe to make the population protected from transmission, otherwise you have rolling waves of vaccinated but infectious people. Which is not avoidable, because...
3) It's everywhere. I think we as a species had a very narrow window to put the genie back in the bottle, but no realistic hope of doing so across all nations. Modern air travel is just a totally new variable in viral pandemics and you cannot vaccinate the entire human race simultaneously, so people flying from Rome to London to NYC will keep reintroducing it to populations. And even if you could, it's a zoonotic disease that is now widespread in many other animal species, including our regional wild white-tail deer. But even if you ALSO drop edible vaccine pods in the woods, COVID seems very good at developing immune escape...
4) Since SARS-CoV-2 evolved in a bat, which has one of the most intense immune systems in the animal kingdom; humans are easy mode. It keeps easily evolving to defeat our immunity and increase its transmissibility, and updated vaccines don't really provide updated protection to the same degree as the original, quasi-sterilizing vaccine. Since it transmits pre-symptomatically, there's no evolutionary pressure to reduce disease severity, and the so-called "milder" Omicron variants are mainly an illusory effect largely due to the population immunity that we had already developed against previous variants by that time. We have never created a durable coronavirus vaccine before, and I'm not entirely sure that even WITH hypothetical frequently-updated, widely-taken nasal boosters that rally a tissue-resident immune response in the airway, we would be able to truly return to a 2019 normal. It would be better, safer, and more stable, certainly...
None of this is to be fatalist in the "well, no use worrying about it then, just gotta live with it" sense. COVID is a chronic society-wrecking event, as the economic/employment and air travel and supply chain chaos has shown from 2020 through today - and there's always the potential a quirk mutation will make it much, much, much worse. Avoiding it is one of the most important things you can do for your short- and long-term health. I don't do indoor dining anymore. I wear a KN95 or N95 or P100 in all indoor settings with mixed households, barring strict post-gathering quarantining and testing. That's "living with" COVID.